
Top 5 Mistakes in MIPS Quality
We tell our clients, “Quality is King.” We focus on this because Quality makes up the largest percentage of your overall Merit-Based Incentive Payment (MIPS) Score, it also means your performance in this category is key to your overall success in the program.
In the 2019 performance year, each Eligible Clinician or group must report 6 quality measures. At least one of these 6 measures must be a “high-priority” or” outcome-based” measure. And the time frame for collecting quality data is all year or in other words the full 365-day performance period from Jan 1 – Dec 31, 2019.
As MIPS consultants, we notice when clients are making one of these five common mistakes and help them course-correct. We’ve outlined the five mistakes below. Are you guilty of any of these?
Mistake 1. You don’t collect data consistently or for enough patients.
When MIPS began there was a key change in the Quality category from programs of the past. They mandated that you not only collect data for Medicare patient but also from ALL the other payers as well. This was a huge challenge early on for many clinicians and groups. The larger problem today though is often what CMS refers to as the 60% “data completeness” requirement in the Quality category. Simply put, it means that when a measure applies to ANY patient in the practice that you are collecting data 60% of the time or more when the patient meets the measure’s denominator specifications. Let’s look at an example of this.
Measure #226: Percentage of patients aged 18 years and older who were screened for tobacco use and received tobacco cessation intervention if identified as a tobacco user.
The denominator specifications for measure 226: All patients aged 18 years and older seen for at least two visits or at least one preventive visit during the measurement period.
That means you or your clinical support team must collect measure data for 60% or more of all patients during the 2019 calendar year who are 18 years and older seen for at least two visits or at least one preventive visit during the measurement period. That’s a whole lot of patients!
It’s important that once you select the measures, you start collecting data right away! We remind our data collection stakeholders in the practice or facility to think “every patient, every measure, and every visit.” This ensures consistency to meet data completeness and offer the most opportunity for performance ratings to meet or exceed benchmarks.
Mistake 2. You select measures without considering overall point potential.
What we’re really talking about here are benchmarks and their corresponding deciles. Measure-specific benchmarks, established based upon a measure’s performance rate two years prior by CMS, determine a clinician’s score on the 10-point scale. These 10 points each have a corresponding decile range.
Deciles are really just the performance range tiers (1-10) that you can be awarded for each measure.
Here’s a picture, because this is just a much easier way to explain it.
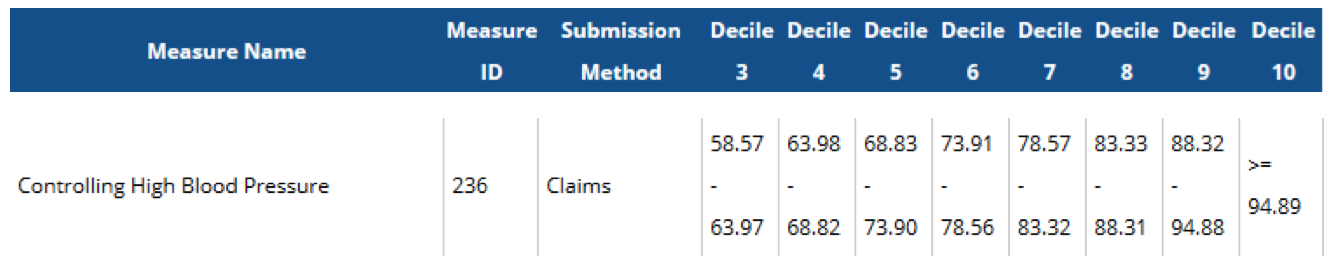
If you were reporting Measure 236: Controlling High Blood Pressure via claims and your overall performance rate was 85.1 percent, you would earn a total of 8 points for this measure.
The bottom line here, if you select a measure you MUST vet the point potential based on the updated and annual publication of deciles. It would be impossible to maximize your “quality” performance if you select 3 new measures, 2 topped out measures and 1 extremely topped out measure. You will earn a score that is mediocre at best before you even get started!
Mistake 3. You selected “easy” measures or the same ones as last year.
Ok, so you heard me say it above. Measure point potential can and will change on an annual basis. When you report the same measures each year (and lots of clinicians do), you want to pay attention to a measure’s status.
Measures can become “topped out “or even “extremely topped out”. Topped-out means that the performance of these measures has become so high, by those that report them that statistically, CMS cannot distinguish the so-so performers from those that did extremely well. Topped out measures that have a benchmark and are topped out for at least two consecutive years can earn up to a maximum of 7 points, instead of 10. This would limit your overall total points possible in the Quality category. Measures determined to be “extremely topped out” with average performance between the 98th and 100th percentile are not subject to the 4-year removal timeline and will ultimately be removed as options.
Similarly, measures with “new” status can become pitfalls when talking about possible points. When a new measure comes out (or an existing measure is slightly changed), it takes two years of data collection to create a formally published benchmark. However, in the meantime, a benchmark may be created under certain circumstances if enough people report enough information based on CMS specific criteria. Since you will have no clue if the scenario above was met, in the case where a benchmark will not be set (because the above criteria were not met), CMS will only award the clinician 3 points. Three out of 10 possible (and much needed) points for overall success can definitely hurt an overall average.
So, buyer beware when it comes to reporting new measures.
Mistake 4. You are collecting and submitting quality data the same way you always have.
There are multiple ways to submit quality measure data to CMS. You can use your EHR, a registry, QCDR, or through claims. There are pros and cons to submitting via certain mechanisms.
While some methods are “free”, others cost money, typically based on the number of clinicians or patients for which you collect data. Certain registries can only submit data on a subset of measures available in the program, which can potentially steer you into a situation with limited measures to choose from that also have limited point potential. On the other hand, a specialty specific registry may offer non-MIPS measures that better align with your clinical scope and patient population. Some registries interface with EHRs without a middle-man. Others require a mapping intermediary which can be problematic and cause additional administrative or operational burden. Some EHRs and registries offer score estimations.
New in 2019, CMS will finally be accepting data from MULTIPLE mechanisms for a single clinician or group. This is great for multi-specialty groups or even those that want to change submission mechanisms mid-year.
The take-away here is that there is no “one size fits all” way to collect and submit quality data. Your strategy should be reviewed on an annual basis.
Mistake 5. You are worried or afraid to report as a Group.
Look, we’ve all been burned by that group project where one kid didn’t do his work. Reporting as a group under a single TIN means that quality becomes a team effort and we need everyone to participate sufficiently and do well. But reporting as a group doesn’t have to be scary. It can actually greatly reduce the administrative burden, give your organization a better return on your investment of time and money to the MIPS program, when it’s all been said and done, reporting as a group can ensure that money is not left on the table. Read more about that here.